Earlier this month, the Centers for Medicare and Medicaid Services released the proposed Medicare Physician Payment rule for 2021 that outlines the agency’s policies and payments for Medicare Part B services.
The public comment on the proposed rule closes Oct. 4, 2020. The ATS will be submitting comments on the proposed rule on behalf of the ATS membership.
Overall Impacts
The impact on physician practices varies by specialty. Those practices that rely on inpatient and procedural services will see the greatest reduction in reimbursement while office-based practices may see an increase in reimbursement. Below is a chart with the CMS 2021 project payment changes by specialty. CMS is projecting pulmonary physicians will see a 1 percent increase in 2021 Medicare payments, while Medicare critical care payments are projected to be cut by 8 percent.
2021 Conversion Factor
The PFS conversion factor is the reimbursement level set by CMS for one relative value unit (RVU) and changes each year, usually in a positive way. Since the repeal of the sustainable growth rate in 2015, health care providers have counted on relative stability in the conversion factor. In 2021, however, the conversion factor will go from $36.09 to $32.26, a 10.61 percent reduction absent congressional action or other legal authorities identified by the White House. CMS predicts a $10.2 billion dollar increase in spending in certain areas and budget neutrality requires this be offset by reductions in other areas. Approximately half of the conversion factor reduction is necessary to pay for the increase in the RVUs related to the revaluing of the office E/M CPT codes and the remainder for other programs and services.
Office Based E/M Services
In the CY 2021 proposed rule CMS has also accepted the RUC recommended changes in code descriptors and levels of reimbursement for office-based E/M codes 99202-99215. The level of these codes will now be determined using medical decision making or time. Please note that CPT code 99201 has been eliminated effective Jan. 1, 2021. The increase in reimbursement for office E/M visits does not apply to the visits that are bundled into global surgery codes. This decision is largely responsible for the projected Medicare reimbursements of surgical specialties.
GPCC1X Add-On Code
As noted in the 2020 final rule, CMS finalized a new E/M add-on code (GPC1X Visit complexity inherent to evaluation and management associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious, or complex chronic condition. (Add - on code, list separately in addition to office/outpatient evaluation and management visit, new or established)) to describe visit complexity. CMS states that this service is distinct from other preventive or care management codes because “GPC1X reflects the time, intensity, and PE when practitioners furnish services that enable them to build longitudinal relationships with all patients (that is, not only those patients who have a chronic condition or single-high risk disease) and to address the majority of patients’ health care needs with consistency and continuity over longer periods of time.” CMS assumes that the specialties which predominantly furnish E/M associated with medical care services that are part of ongoing care related to a patient’s single, serious, or complex condition will bill the add-on code with every E/M visit. Total utilization for the code across all specialties is estimated to be $181M. ATS members should learn how to appropriately bill for this new GPCC1X service.
Proposed RVUs and National Unadjusted PFS Rates for Office/Outpatient E/M Visits
| CPT code | 2020 time | 2020 RVU | Proposed 2021 time | Proposed 2021 RVU |
|---|---|---|---|---|
| 99201 | 17 | 0.48 | NA | NA |
| 99202 | 22 | 0.93 | 22 | 0.93 |
| 99203 | 29 | 1.42 | 40 | 1.6 |
| 99204 | 45 | 2.43 | 60 | 2.6 |
| 99205 | 67 | 3.17 | 85 | 3.5 |
| 99211 | 7 | 0.18 | 7 | 0.18 |
| 99212 | 16 | 0.48 | 18 | 0.70 |
| 99213 | 23 | 0.97 | 30 | 1.30 |
| 99214 | 40 | 1.50 | 49 | 1.92 |
| 99215 | 55 | 2.11 | 70 | 2.8 |
| 99XXX | NA | NA | 15 | 0.61 |
CPT code 99XXX represents a prolonged service code that should be used when one uses time to determine the level of a code and exceeds the time of codes 99205 and 99215. While CMS accepted the RVU values of the 99XXX code, it also changed the time elements for reporting.
| New Patient Office/Outpatient E/M Visit (Total Practitioner Time, When Time is Used to Select Code Level) |
CPT code |
|---|---|
| 60-74 minutes | 99205 |
| 89-103 minutes | 99205 x1 and 99XXX x1 |
| 104-118 minutes | 99205 x1 and 99XXX x2 |
| 119 or more minutes | 99205 x1 and 99XXX x3 or more for each additional 15 minutes |
| Established Patient Office/Outpatient E/M Visit (Total Practitioner Time, When Time is Used to Select Code Level) |
|
|---|---|
| 40-54 minutes | 99215 |
| 69-83 minutes | 99215 x1 and 99XXX x1 |
| 84-98 minutes | 99215 x1 and 99XXX x2 |
| 99 or more minutes | 99215 x1 and 99XXX x3 or more for each additional 15 minutes |
The proposed rule includes significant increases in the RVU values of the E/M codes at the higher levels and, as noted above, this increase is responsible for a large share of the reduction in the conversion factor.
Proposed RVUs and National Unadjusted PFS Rates for Office/Outpatient E/M Visits
| HCPCS Code | Work | Non-Facility PE | Facility PE | Mal-practice | Total Non-Facility | Total Facility | Non-facility Rate | Facility Rate |
|---|---|---|---|---|---|---|---|---|
| 99202 | 0.93 | 1.12 | 0.41 | 0.09 | 2.14 | 1.43 | $69.04 | $46.13 |
| 99203 | 1.60 | 1.54 | 0.67 | 0.15 | 3.29 | 2.42 | $106.14 | $78.07 |
| 99204 | 2.60 | 2.10 | 1.12 | 0.24 | 4.94 | 3.96 | $159.37 | $127.75 |
| 99205 | 3.50 | 2.71 | 1.57 | 0.32 | 6.53 | 5.39 | $210.66 | $173.88 |
| 99211 | 0.18 | 0.50 | 0.08 | 0.01 | 0.69 | 0.27 | $22.26 | $8.71 |
| 99212 | 0.70 | 0.91 | 0.29 | 0.07 | 1.68 | 1.06 | $54.20 | $34.20 |
| 99213 | 1.30 | 1.29 | 0.56 | 0.10 | 2.69 | 1.96 | $86.78 | $63.23 |
| 99214 | 1.92 | 1.76 | 0.84 | 0.13 | 3.81 | 2.89 | $122.91 | $93.23 |
| 99215 | 2.80 | 2.33 | 1.26 | 0.21 | 5.34 | 4.27 | $172.27 | $137.75 |
| 99XXX | 0.61 | 0.31 | 0.28 | 0.05 | 0.97 | 0.94 | $31.29 | $30.32 |
| GPC1X | 0.33 | 0.14 | 0.14 | 0.02 | 0.49 | 0.49 | $15.81 | $15.81 |
Accepted RUC Values
The proposed rule also includes a number of physician work revaluation of pulmonary services including, spirometry (CPT 94101) and exercise testing (CPT 946X0, 94617, 94618, and 94621) The ATS is pleased that CMS accepted physician work values recommended by the ATS and AMA RUC for these codes.
Critical Care Payment Cuts
The ATS is extremely concerned with the projected Medicare cuts in critical care reimbursement, particularly in the midst of a COVID-19 pandemic and the added costs, risk and demands placed on critical care providers. The cuts to critical care are not driven by any changes in critical care but are entirely driven by the Medicare budget neutrality requirements. In short, the increased payments in E/M offices visit and primary care payments are offset by cuts to every other service, including critical care. The ATS has reached out to CMS to express our concern with the critical care cuts and will coordinate peer organizations to urge CMS to protect critical care providers from these steep payment cuts.
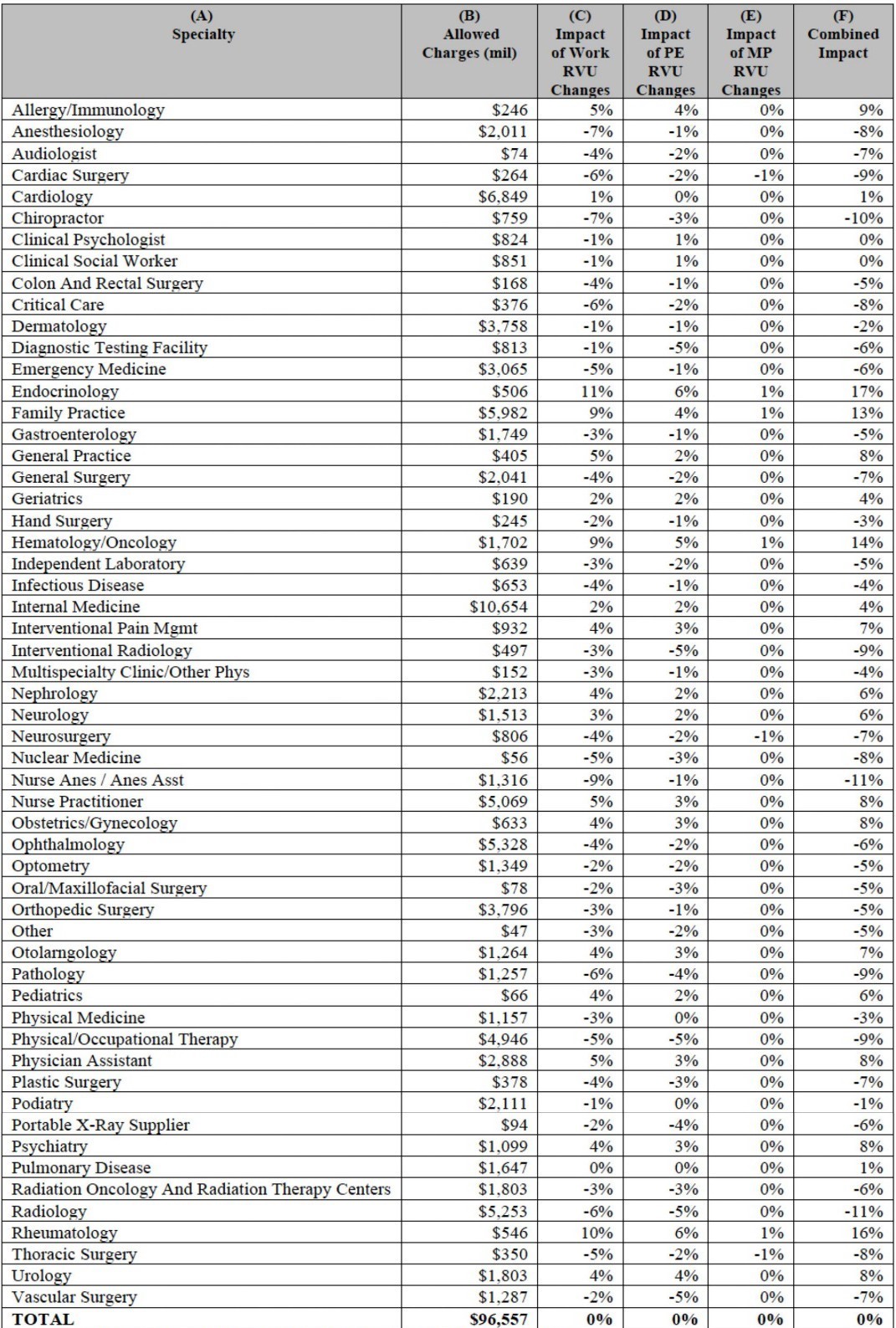
*Column F may not equal the sum of columns C, D, and E due to rounding.
